



























-
 Traditional Vital Signs WorkflowThe traditional vital signs workflow is a common setup for family practices or physician offices. Patient weight and height are captured manually while leading the patient to the exam room, which can cause delays with patient flow in the hallway. Pulse, temperature and blood pressure are taken manually inside the exam room.
Traditional Vital Signs WorkflowThe traditional vital signs workflow is a common setup for family practices or physician offices. Patient weight and height are captured manually while leading the patient to the exam room, which can cause delays with patient flow in the hallway. Pulse, temperature and blood pressure are taken manually inside the exam room.- Vital Signs
- Clinical Process Improvement
- Real-Time Locating System
- EMR Connectivity
- Better Blood Pressure
- Infection Prevention
- Americans with Disabilities
- Single Pane of Glass
-
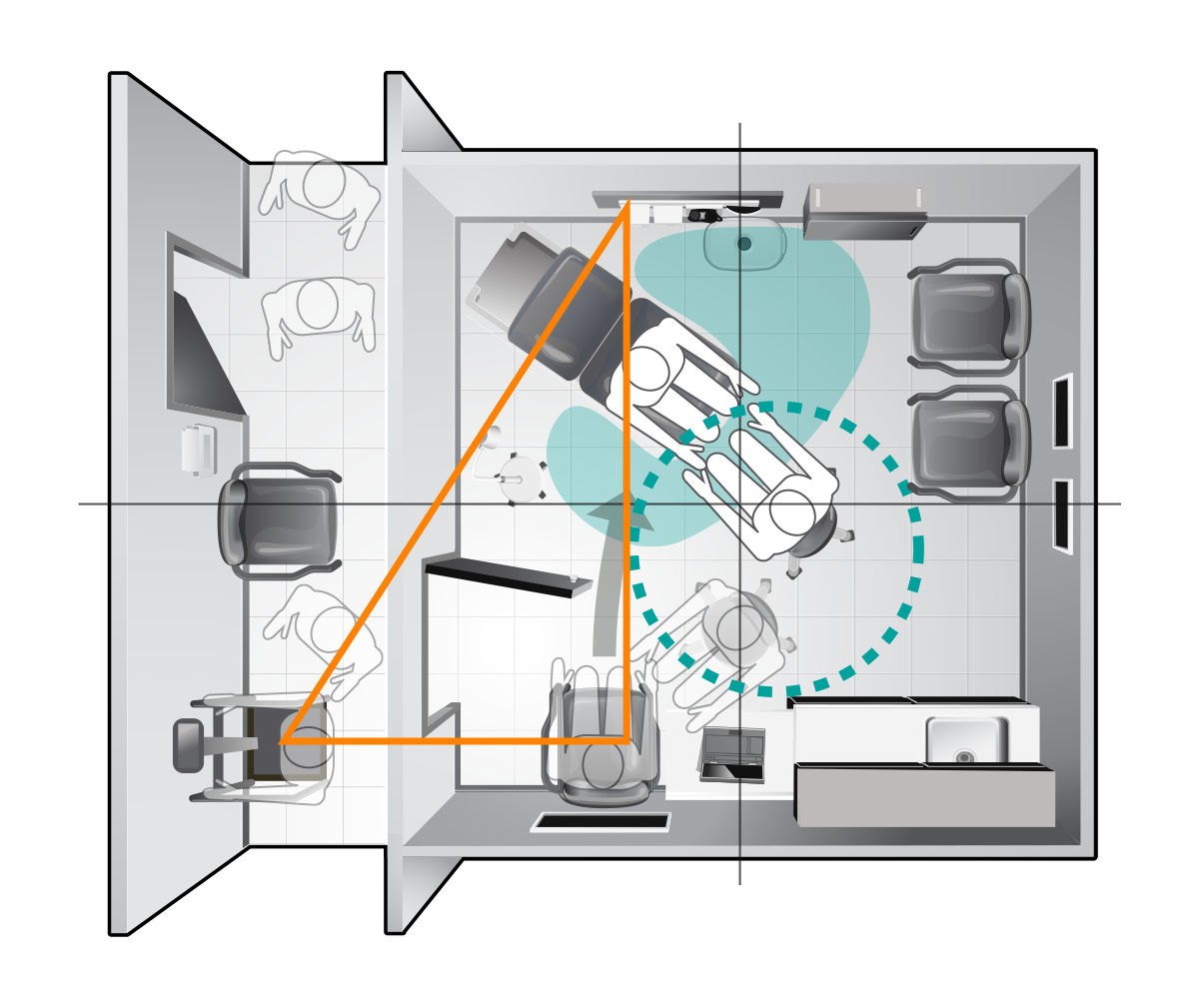 Traditional Vital SignsAfter weight and height are measured in the hallway, the patient is escorted to the exam room and directed to a side chair or the exam table. If the blood pressure cuff is manual and not attached to the wall, the patient is seated on a table or in a side chair next to the work surface for paper-based patient records.
Traditional Vital SignsAfter weight and height are measured in the hallway, the patient is escorted to the exam room and directed to a side chair or the exam table. If the blood pressure cuff is manual and not attached to the wall, the patient is seated on a table or in a side chair next to the work surface for paper-based patient records. -
 Time SavingsThe traditional workflow requires an average of 187 seconds from the time the patient is called through vital signs acquisition.
Time SavingsThe traditional workflow requires an average of 187 seconds from the time the patient is called through vital signs acquisition.
-
 Vital Signs
Vital Signs
-
 Clinical Process Improvement
Clinical Process Improvement
-
 Single Pane of Glass
Single Pane of Glass
-
 Infection Prevention
Infection Prevention
-
 Real-Time Locating System
Real-Time Locating System
-
 Americans with Disabilities
Americans with Disabilities
-
 Better Blood Pressure
Better Blood Pressure
-
 EMR Connectivity
EMR Connectivity
Vital signs measurements are captured in multiple locations manually, requiring 187 seconds per patient.
Weight is captured outside of the exam space causing privacy concerns and bottlenecks
Lack of visibility to real-time operations or patient self-rooming workflow inhibits waste reduction efforts.
Disconnected equipment operates autonomously, increasing the likelihood of human error.
The non-adjustable exam table does not support proper patient positioning for accurate BP measurements.
Lack of patient self-rooming as well as capturing vital signs and weight in multiple locations increases the risk of exposure to contagions. Lack of RTLS makes contact tracing a tedious manual process. The exam table cannot be easily moved for cleaning and disinfecting.
Inaccessible exam table poses patient and staff safety risks.
Disconnected devices require manual entry of patient data.
Vital signs measurements are captured in multiple locations manually, requiring 187 seconds per patient.
Weight is captured outside of the exam space causing privacy concerns and bottlenecks
Lack of visibility to real-time operations or patient self-rooming workflow inhibits waste reduction efforts.
Disconnected equipment operates autonomously, increasing the likelihood of human error.
The non-adjustable exam table does not support proper patient positioning for accurate BP measurements.
Lack of patient self-rooming as well as capturing vital signs and weight in multiple locations increases the risk of exposure to contagions. Lack of RTLS makes contact tracing a tedious manual process. The exam table cannot be easily moved for cleaning and disinfecting.
Inaccessible exam table poses patient and staff safety risks.
Disconnected devices require manual entry of patient data.
Vital signs measurements are captured in multiple locations manually, requiring 187 seconds per patient.
Weight is captured outside of the exam space causing privacy concerns and bottlenecks
Lack of visibility to real-time operations or patient self-rooming workflow inhibits waste reduction efforts.
Disconnected equipment operates autonomously, increasing the likelihood of human error.
The non-adjustable exam table does not support proper patient positioning for accurate BP measurements.
Lack of patient self-rooming as well as capturing vital signs and weight in multiple locations increases the risk of exposure to contagions. Lack of RTLS makes contact tracing a tedious manual process. The exam table cannot be easily moved for cleaning and disinfecting.
Inaccessible exam table poses patient and staff safety risks.
Disconnected devices require manual entry of patient data.